Do I Suffer From Over-Pronation Of The Feet
Overview
Over-pronation occurs when the foot collapses too far inward stressing the plantar fascia (the area underneath the arch of the foot.) Normally, one pronates every time he/she walks, but excessive pronation is called over-pronation. When this occurs it can cause pain in the feet, knees, hips, low back and even the shoulder.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Over-pronation is a condition where the arch flattens out which makes the feet roll inward while walking. This condition is also known as flat feet. It imposes extreme additional stresses on the plantar fascia, a fibrous band of tissue which connects the heel to the forefoot. Over-pronation makes walking a painful experience because of the additional strain on the calves, heel and/or back. Treatment for over-pronation involves the use of specially-made orthotics which offers arch support and medial rear foot posting as corrective measures.
Diagnosis
You can test for pronation by looking at the leg and foot from the back. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.
Non Surgical Treatment
If a young child is diagnosed with overpronation braces and custom orthotics can be, conjunction with strengthening and stretching exercises, to realign the bones of the foot. These treatments may have to continue until the child has stopped growing, and orthotics may need to be worn for life in order to prevent the foot reverting to an overpronated state. Wearing shoes that properly support the foot, particularly the arch, is one of the most effective treatments for overpronation. Custom-made orthotic inserts can also be very beneficial. They too support the arch and distribute body weight correctly throughout the foot. Motion-control shoes that prohibit pronation can be worn, so may be useful for those with severe overpronation. One good treatment is to walk barefoot as often as possible. Not relying on shoes to support the arch will encourage proper muscle use. Practicing yoga can help to correct poor posture and teach you how to stand with your weight balanced evenly across the whole foot.
Surgical Treatment
The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain.
Over-pronation occurs when the foot collapses too far inward stressing the plantar fascia (the area underneath the arch of the foot.) Normally, one pronates every time he/she walks, but excessive pronation is called over-pronation. When this occurs it can cause pain in the feet, knees, hips, low back and even the shoulder.
Causes
Generally fallen arches are a condition inherited from one or both parents. In addition, age, obesity, and pregnancy cause our arches to collapse. Being in a job that requires long hours of standing and/or walking (e.g. teaching, retail, hospitality, building etc) contributes to this condition, especially when standing on hard surfaces like concrete floors. Last, but not least unsupportive footwear makes our feet roll in more than they should.
Symptoms
Over-pronation is a condition where the arch flattens out which makes the feet roll inward while walking. This condition is also known as flat feet. It imposes extreme additional stresses on the plantar fascia, a fibrous band of tissue which connects the heel to the forefoot. Over-pronation makes walking a painful experience because of the additional strain on the calves, heel and/or back. Treatment for over-pronation involves the use of specially-made orthotics which offers arch support and medial rear foot posting as corrective measures.
Diagnosis
You can test for pronation by looking at the leg and foot from the back. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.
Non Surgical Treatment
If a young child is diagnosed with overpronation braces and custom orthotics can be, conjunction with strengthening and stretching exercises, to realign the bones of the foot. These treatments may have to continue until the child has stopped growing, and orthotics may need to be worn for life in order to prevent the foot reverting to an overpronated state. Wearing shoes that properly support the foot, particularly the arch, is one of the most effective treatments for overpronation. Custom-made orthotic inserts can also be very beneficial. They too support the arch and distribute body weight correctly throughout the foot. Motion-control shoes that prohibit pronation can be worn, so may be useful for those with severe overpronation. One good treatment is to walk barefoot as often as possible. Not relying on shoes to support the arch will encourage proper muscle use. Practicing yoga can help to correct poor posture and teach you how to stand with your weight balanced evenly across the whole foot.
Surgical Treatment
The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain.
What Are The Main Causes Of Severs Disease?
Overview
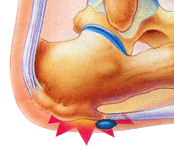
Sever's disease is a pain that occurs in the back of the heel of physically active children at around the time of puberty. Sever's disease occurs due to an inflammation of the growth plate due to excessive pull of the achilles tendon on this growth plate. During puberty the bones quite often grow faster than the muscles and tendons causing the tendons to become tight, this tightness then results in excessive pull on the back of the heel resulting in this painful condition.
Causes
Heel pain is very common in children due to the fact they are cnstantly growing. In most children, the heel bone (the calcaneus) is not fully developed until the age of 14 or older. Until then, new bone is forming at the growth plate of the foot (the apophysis, located at the back of the heel), an area which is softer than others due to its role in accommodating the growth. Repetitive stress on the growth plate due to walking, running and sports causes inflammation in the heel area. Because the heel's growth plate is sensitive, repeated running and pounding on hard surfaces can result in pediatric heel pain. Children and adolescents who take part in a lot of sport are especially vulnerable. Over-pronation (fallen arches and rolling inwards of the feet) will increase the impact on the growth plate and is therefore a significant cause and a major contributing factor to heel pain in children.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include Pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, Worsening of pain after exercise, A tender swelling or bulge on the heel that is sore to touch, Calf muscle stiffness first thing in the morning, Limping, A tendency to tiptoe.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
Treatment of Severs disease usually involves a combination of an accurate analysis of your child?s gait, muscles, tendons, ligaments and joints is a crucial first step. Specific stretching and strengthening exercises often make up part of the treatment. Anti-inflammatory measures such as ice baths after exercise can be helpful in the short term. Footwear review, assessment and advice is important. Orthotic devices are often needed to firstly control any abnormal traction or tension on the heel growth plate and, secondly, too unload the ground reaction forces on the heel bone. Podiatry Care has podiatrists with specific paediatric training enabling them to utilise treatment options to relieve heel pain in children very quickly. If your child is struggling to play sport, see a Podiatry Care podiatrist near you. In severe cases modification to activity levels may be required. Treatment of Severs disease does NOT require surgery. This foot condition responds very well to conservative treatment.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Sever's disease is a pain that occurs in the back of the heel of physically active children at around the time of puberty. Sever's disease occurs due to an inflammation of the growth plate due to excessive pull of the achilles tendon on this growth plate. During puberty the bones quite often grow faster than the muscles and tendons causing the tendons to become tight, this tightness then results in excessive pull on the back of the heel resulting in this painful condition.
Causes
Heel pain is very common in children due to the fact they are cnstantly growing. In most children, the heel bone (the calcaneus) is not fully developed until the age of 14 or older. Until then, new bone is forming at the growth plate of the foot (the apophysis, located at the back of the heel), an area which is softer than others due to its role in accommodating the growth. Repetitive stress on the growth plate due to walking, running and sports causes inflammation in the heel area. Because the heel's growth plate is sensitive, repeated running and pounding on hard surfaces can result in pediatric heel pain. Children and adolescents who take part in a lot of sport are especially vulnerable. Over-pronation (fallen arches and rolling inwards of the feet) will increase the impact on the growth plate and is therefore a significant cause and a major contributing factor to heel pain in children.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include Pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, Worsening of pain after exercise, A tender swelling or bulge on the heel that is sore to touch, Calf muscle stiffness first thing in the morning, Limping, A tendency to tiptoe.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
Treatment of Severs disease usually involves a combination of an accurate analysis of your child?s gait, muscles, tendons, ligaments and joints is a crucial first step. Specific stretching and strengthening exercises often make up part of the treatment. Anti-inflammatory measures such as ice baths after exercise can be helpful in the short term. Footwear review, assessment and advice is important. Orthotic devices are often needed to firstly control any abnormal traction or tension on the heel growth plate and, secondly, too unload the ground reaction forces on the heel bone. Podiatry Care has podiatrists with specific paediatric training enabling them to utilise treatment options to relieve heel pain in children very quickly. If your child is struggling to play sport, see a Podiatry Care podiatrist near you. In severe cases modification to activity levels may be required. Treatment of Severs disease does NOT require surgery. This foot condition responds very well to conservative treatment.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Causes Indicators And Treatment Of Achilles Tendon Ruptures
Overview
 Your Achilles tendon is a large band of tissue in the back of your ankle. It connects your calf muscles to your heel bone. The tendon helps you point your foot downward, rise on your toes, and push off when you walk. You use it almost every time you move. But repeated stress can make the tendon more prone to injury. It may become inflamed and develop small tears (tendonitis). A complete tear through the tendon is known as an Achilles tendon rupture.
Your Achilles tendon is a large band of tissue in the back of your ankle. It connects your calf muscles to your heel bone. The tendon helps you point your foot downward, rise on your toes, and push off when you walk. You use it almost every time you move. But repeated stress can make the tendon more prone to injury. It may become inflamed and develop small tears (tendonitis). A complete tear through the tendon is known as an Achilles tendon rupture.
Causes
An Achilles tendon rupture is often caused by overstretching the tendon. This typically occurs during intense physical activity, such as running or playing basketball. Pushing off from the foot while the knee is straight, pivoting, jumping, and running are all movements that can overstretch the Achilles tendon and cause it to rupture. A rupture can also occur as the result of trauma that causes an over-stretching of the tendon, such as suddenly tripping or falling from a significant height. The Achilles tendon is particularly susceptible to injury if it is already weak. Therefore, individuals who have a history of tendinitis or tendinosis are more prone to a tendon rupture. Similarly, individuals who have arthritis and overcompensate for their joint pain by putting more stress on the Achilles tendon may also be more susceptible to an Achilles tendon rupture.
Symptoms
You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are a flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later. A person with a ruptured Achilles tendon may experience one or more of the following. Sudden pain (which feels like a kick or a stab) in the back of the ankle or calf, often subsiding into a dull ache. A popping or snapping sensation. Swelling on the back of the leg between the heel and the calf. Difficulty walking (especially upstairs or uphill) and difficulty rising up on the toes.
Diagnosis
A physician usually can make this diagnosis with a good physical examination and history. X-rays usually are not taken. A simple test of squeezing the calf muscles while lying on your stomach should indicate if the tendon is still connected (the foot should point). This test isolates the connection between the calf muscle and tendon and eliminates other tendons that may still allow weak movement. A word of caution, Achilles tendon rupture is often misdiagnosed as a strain or minor tendon injury. Swelling and the continuing ability to weakly point your toes can confuse the diagnosis. Ultrasound and MRI are tests that can assist in difficult diagnosis. Depending on the degree of injury, these tests can also assist in determining which treatment may be best.
Non Surgical Treatment
Nonsurgical treatment involves extended casting, special braces, orthotics, and physical therapy. Avoids the normal complications and expenses of surgery. Some studies show the outcome is similar to surgery in regard to strength and function. There is risk of an over-lengthened tendon with inadequate tension. Extended immobilization can lead to more muscle weakness. Nonsurgical treatment has a higher incidence of re-rupture than surgical repair. Nonsurgical treatment is often used for nonathletes or for those with a general low level of physical activity who would not benefit from surgery. The elderly and those with complicating medical conditions should also consider conservative nonsurgical treatment. 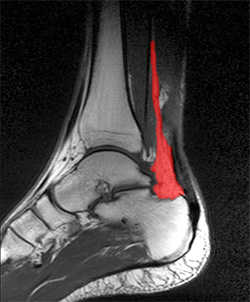
Surgical Treatment
A completely ruptured Achilles tendon requires surgery and up to 12 weeks in a cast. Partial tears are sometimes are treated with surgery following by a cast. Because the tendon shortens as it heals, a heel lift is used for 6 months or more after the cast comes off. Physical therapy to regain flexibility and then strength are begun as soon as the cast is off.
Prevention
To help reduce your chance of getting Achilles tendon rupture, take the following steps. Do warm-up exercises before an activity and cool down exercises after an activity. Wear proper footwear. Maintain a healthy weight. Rest if you feel pain during an activity. Change your routine. Switch between high-impact activities and low-impact activities. Strengthen your calf muscle with exercises.
Functional Leg Length Discrepancy Way Of Measuring
Overview
Leg length discrepancy is an orthopaedic problem that usually appears in childhood, in which one's two legs are of unequal lengths. Often abbreviated as ?LLD,' leg length discrepancy may be caused by or associated with a number of other orthopaedic or medical conditions, but is generally treated in a similar fashion, regardless of cause and depending on severity. Leg length discrepancy is sometimes divided up into 'true LLD' and 'functional LLD.' Functional LLD occurs when the legs are actually equal in length, but some other condition, such as pelvic obliquity (a tilt in the position of the pelvis), creates the appearance of legs of different lengths.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
You may be prescribed a heel lift, which will equal out your leg length and decrease stress on your low back and legs. If it?s your pelvis causing the leg length discrepancy, then your physical therapist could use your muscles to realign your pelvis and then strengthen your core/abdominal region to minimize the risk of such malalignment happening again. If you think that one leg may be longer than the other and it is causing you to have pain or you are just curious, then make an appointment with a physical therapist.

Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
Leg length discrepancy is an orthopaedic problem that usually appears in childhood, in which one's two legs are of unequal lengths. Often abbreviated as ?LLD,' leg length discrepancy may be caused by or associated with a number of other orthopaedic or medical conditions, but is generally treated in a similar fashion, regardless of cause and depending on severity. Leg length discrepancy is sometimes divided up into 'true LLD' and 'functional LLD.' Functional LLD occurs when the legs are actually equal in length, but some other condition, such as pelvic obliquity (a tilt in the position of the pelvis), creates the appearance of legs of different lengths.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
You may be prescribed a heel lift, which will equal out your leg length and decrease stress on your low back and legs. If it?s your pelvis causing the leg length discrepancy, then your physical therapist could use your muscles to realign your pelvis and then strengthen your core/abdominal region to minimize the risk of such malalignment happening again. If you think that one leg may be longer than the other and it is causing you to have pain or you are just curious, then make an appointment with a physical therapist.
Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
Does Posterior Tibial Tendon Dysfunction (PTTD) Require Surgical Teatments ?
Overview
When we have foot pain, it isn?t always easy to pinpoint the source because we can?t visualize the structure of all the bones, muscles, and tendons on the inside. The posterior tibial tendon plays an important supportive role within the structure of the foot. It attaches to your calf muscle and then comes down along the inside of your ankle, connecting to the bones inside your foot at the other side. This tendon?s main function is to hold up your arch and support your foot during each and every movement. Every step, run, walk, or jump is made possible with the support from this crucial tendon. While it is designed to perform such an important role, it is vulnerable to stress and injury. A tear during a traumatic injury or stress from overuse can injure the tissues within the tendon. This kind of injury is referred to as posterior tibial tendon dysfunction (PTTD). A really hard fall during a sports game or exposure to a repetitive motion, such as the impact on feet during soccer, tennis, football or basketball, can cause an injury. Flat foot and flat feet in adults can exacerbate this condition. The tendon can experience small tears and become inflamed. If the inflammation is allowed to continue and worsen over time, it will weaken further and could rupture completely. 
Causes
Adult flatfoot typically occurs very gradually. If often develops in an obese person who already has somewhat flat feet. As the person ages, the tendons and ligaments that support the foot begin to lose their strength and elasticity.
Symptoms
Often, this condition is only present in one foot, but it can affect both. Adult acquired flatfoot symptoms vary, but can swelling of the foot's inner side and aching heel and arch pain. Some patients experience no pain, but others may experience severe pain. Symptoms may increase during long periods of standing, resulting in fatigue. Symptoms may change over time as the condition worsens. The pain may move to the foot's outer side, and some patients may develop arthritis in the ankle and foot.
Diagnosis
Posterior Tibial Tendon Dysfunction is diagnosed with careful clinical observation of the patient?s gait (walking), range of motion testing for the foot and ankle joints, and diagnostic imaging. People with flatfoot deformity walk with the heel angled outward, also called over-pronation. Although it is normal for the arch to impact the ground for shock absorption, people with PTTD have an arch that fully collapses to the ground and does not reform an arch during the entire gait period. After evaluating the ambulation pattern, the foot and ankle range of motion should be tested. Usually the affected foot will have decreased motion to the ankle joint and the hindfoot. Muscle strength may also be weaker as well. An easy test to perform for PTTD is the single heel raise where the patient is asked to raise up on the ball of his or her effected foot. A normal foot type can lift up on the toes without pain and the heel will invert slightly once the person has fully raised the heel up during the test. In early phases of PTTD the patient may be able to lift up the heel but the heel will not invert. An elongated or torn posterior tibial tendon, which is a mid to late finding of PTTD, will prohibit the patient from fully rising up on the heel and will cause intense pain to the arch. Finally diagnostic imaging, although used alone cannot diagnose PTTD, can provide additional information for an accurate diagnosis of flatfoot deformity. Xrays of the foot can show the practitioner important angular relationships of the hindfoot and forefoot which help diagnose flatfoot deformity. Most of the time, an MRI is not needed to diagnose PTTD but is a tool that should be considered in advanced cases of flatfoot deformity. If a partial tear of the posterior tibial tendon is of concern, then an MRI can show the anatomic location of the tear and the extensiveness of the injury.
Non surgical Treatment
Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities. In many cases of PTTD, treatment can begin with non-surgical approaches that may include. Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support. 
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. (See surgical correction of adult acquired flatfoot). Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot - meaning you will be on crutches for two months. The bottom line is, Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention.
What Causes Posterior Tibial Tendon Dysfunction ?
Overview
Acquired flatfoot deformity caused by dysfunction of the posterior tibial tendon is a common clinical problem. Treatment, which depends on the severity of the symptoms and the stage of the disease, includes non-operative options, such as rest, administration of anti-inflammatory medication, and immobilization, as well as operative options, such as tendon transfer, calcaneal osteotomy, and several methods of arthrodesis. 
Causes
Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity.
Symptoms
Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot.
Diagnosis
The history and physical examination are probably the most important tools the physician uses to diagnose this problem. The wear pattern on your shoes can offer some helpful clues. Muscle testing helps identify any areas of weakness or muscle impairment. This should be done in both the weight bearing and nonweight bearing positions. A very effective test is the single heel raise. You will be asked to stand on one foot and rise up on your toes. You should be able to lift your heel off the ground easily while keeping the calcaneus (heel bone) in the middle with slight inversion (turned inward). X-rays are often used to study the position, shape, and alignment of the bones in the feet and ankles. Magnetic resonance (MR) imaging is the imaging modality of choice for evaluating the posterior tibial tendon and spring ligament complex.
Non surgical Treatment
Flatfoot deformity can be treated conservatively or with surgical intervention depending on the severity of the condition. When people notice their arches flattening, they should immediately avoid non-supportive shoes such as flip-flops, sandals or thin-soled tennis shoes. Theses shoes will only worsen the flatfoot deformity and exacerbate arch pain. Next, custom orthotics are essential for people with collapsed arches. Over-the-counter insoles only provide cushion and padding to the arch, whereas custom orthotics are fabricated to specifically fit the patient?s foot and provide support in the arch where the posterior tibial tendon is unable to anymore. Use of custom orthotics in the early phases of flatfoot or PTTD can prevent worsening of symptoms and prevent further attenuation or injury to the posterior tibial tendon. In more severe cases of flatfoot deformity an ankle foot orthosis (AFO) such as a Ritchie brace is needed. This brace provides more support to the arch and hindfoot rather than an orthotic but can be bulky in normal shoegear. Additional treatment along with use of custom orthotics is use of non-steroidal anti-inflammatories (NSAIDS) such as Advil, Motrin, or Ibuprofen which can decrease inflammation to the posterior tibial tendon. If pain is severe, the patient may need to be placed in a below the knee air walker boot for several weeks which will allow the tendon to rest and heal, especially if a posterior tibial tendon tear is noted on MRI. 
Surgical Treatment
Until recently, operative treatment was indicated for most patients with stage 2 deformities. However, with the use of potentially effective nonoperative management , operative treatment is now indicated for those patients that have failed nonoperative management. The principles of operative treatment of stage 2 deformities include transferring another tendon to help serve the role of the dysfunctional posterior tibial tendon (usually the flexor hallucis longus is transferred). Restoring the shape and alignment of the foot. This moves the weight bearing axis back to the center of the ankle. Changing the shape of the foot can be achieved by one or more of the following procedures. Cutting the heel bone and shifting it to the inside (Medializing calcaneal osteotomy). Lateral column lengthening restores the arch and overall alignment of the foot. Medial column stabilization. This stiffens the ray of the big toe to better support the arch. Lengthening of the Achilles tendon or Gastrocnemius. This will allow the ankle to move adequately once the alignment of the foot is corrected. Stage 3 acquired adult flatfoot deformity is treated operatively with a hindfoot fusion (arthrodesis). This is done with either a double or triple arthrodesis - fusion of two or three of the joints in hindfoot through which the deformity occurs. It is important when a hindfoot arthrodesis is performed that it be done in such a way that the underlying foot deformity is corrected first. Simply fusing the hindfoot joints in place is no longer acceptable.
What Are The Main Causes Of Posterior Tibial Tendon Dysfunction ?
Overview Often considered solely a product of genetics, flatfoot rarely carries with it the stigma of presenting over time. The truth, however, is that flatfoot does not discriminate on the basis of age and can become an issue in the form of adult-acquired flatfoot. Like its congenital cousin, adult-acquired flatfoot deformity is one that, in causing structural damage to the foot (and particularly to the posterior tibial tendon), creates an imbalance that may result in any number of symptoms, including inflammation, pain, stiffness, limited mobility, and even arthritis.  Causes Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. Symptoms The first stage represents inflammation and symptoms originating from an irritated posterior tibial tendon, which is still functional. Stage two is characterized by a change in the alignment of the foot noted on observation while standing (see above photos). The deformity is supple meaning the foot is freely movable and a ?normal? position can be restored by the examiner. Stage two is also associated with the inability to perform a single-leg heel rise. The third stage is dysfunction of the posterior tibial tendon is a flatfoot deformity that becomes stiff because of arthritis. Prolonged deformity causes irritation to the involved joints resulting in arthritis. The fourth phase is a flatfoot deformity either supple (stage two) or stiff (stage 3) with involvement of the ankle joint. This occurs when the deltoid ligament, the major supporting structure on the inside of the ankle, fails to provide support. The ankle becomes unstable and will demonstrate a tilted appearance on X-ray. Failure of the deltoid ligament results from an inward displacement of the weight bearing forces. When prolonged, this change can lead to ankle arthritis. The vast majority of patients with acquired adult flatfoot deformity are stage 2 by the time they seek treatment from a physician. Diagnosis Starting from the knee down, check for any bowing of the tibia. A tibial varum will cause increased medial stress on the foot and ankle. This is essential to consider in surgical planning. Check the gastrocnemius muscle and Achilles complex via a straight and bent knee check for equinus. If the range of motion improves to at least neutral with bent knee testing of the Achilles complex, one may consider a gastrocnemius recession. If the Achilles complex is still tight with bent knee testing, an Achilles lengthening may be necessary. Check the posterior tibial muscle along its entire course. Palpate the muscle and observe the tendon for strength with a plantarflexion and inversion stress test. Check the flexor muscles for strength in order to see if an adequate transfer tendon is available. Check the anterior tibial tendon for size and strength. Non surgical Treatment There are many non-surgical options for the flatfoot. Orthotics, non-custom braces, shoe gear changes and custom braces are all options for treatment. A course of physical therapy may be prescribed if tendon inflammation is part of the problem. Many people are successfully treated with non-surgical alternatives.
Causes Many health conditions can create a painful flatfoot, an injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. Symptoms The first stage represents inflammation and symptoms originating from an irritated posterior tibial tendon, which is still functional. Stage two is characterized by a change in the alignment of the foot noted on observation while standing (see above photos). The deformity is supple meaning the foot is freely movable and a ?normal? position can be restored by the examiner. Stage two is also associated with the inability to perform a single-leg heel rise. The third stage is dysfunction of the posterior tibial tendon is a flatfoot deformity that becomes stiff because of arthritis. Prolonged deformity causes irritation to the involved joints resulting in arthritis. The fourth phase is a flatfoot deformity either supple (stage two) or stiff (stage 3) with involvement of the ankle joint. This occurs when the deltoid ligament, the major supporting structure on the inside of the ankle, fails to provide support. The ankle becomes unstable and will demonstrate a tilted appearance on X-ray. Failure of the deltoid ligament results from an inward displacement of the weight bearing forces. When prolonged, this change can lead to ankle arthritis. The vast majority of patients with acquired adult flatfoot deformity are stage 2 by the time they seek treatment from a physician. Diagnosis Starting from the knee down, check for any bowing of the tibia. A tibial varum will cause increased medial stress on the foot and ankle. This is essential to consider in surgical planning. Check the gastrocnemius muscle and Achilles complex via a straight and bent knee check for equinus. If the range of motion improves to at least neutral with bent knee testing of the Achilles complex, one may consider a gastrocnemius recession. If the Achilles complex is still tight with bent knee testing, an Achilles lengthening may be necessary. Check the posterior tibial muscle along its entire course. Palpate the muscle and observe the tendon for strength with a plantarflexion and inversion stress test. Check the flexor muscles for strength in order to see if an adequate transfer tendon is available. Check the anterior tibial tendon for size and strength. Non surgical Treatment There are many non-surgical options for the flatfoot. Orthotics, non-custom braces, shoe gear changes and custom braces are all options for treatment. A course of physical therapy may be prescribed if tendon inflammation is part of the problem. Many people are successfully treated with non-surgical alternatives.  Surgical Treatment For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Surgical Treatment For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.